
Isolated osteoarthritis of the Patello-Femoral Joint (PFJ) is a common source of pain and disability for a wide range of patients. It can affect patients in their teens all the way through adulthood. In most cases, the osteoarthritis develops as a consequence of patello-femoral maltracking, dysplasia or imbalance, and has often been associated with anterior knee pain or instability for most of the patient’s adult life. There is often a strong family history, and it is not uncommon to treat 3 generations of the same family with different stages of the condition.
SYMPTOMS
Symptoms can vary widely, with radiological signs often correlating poorly with symptoms. Patients will usually complain of anterior knee pain, particularly when loading the PFJ. Such activities include stair and hill climbing, often with symptoms worse on descent. Transfer pain, when getting into or out of a chair is common. Characteristically, walking or even running on flat surfaces does not result in much pain. As symptoms become severe falls are not uncommon, particularly in the elderly, due to very inefficient and painful patella-femoral function.
SIGNS
There are a wide variety of signs including knee effusion, patella-femoral crepitus, synovitis, patellar instability.
TREATMENT OPTIONS
Non Operative
- Weight reduction: The PFJ takes 3-5 times body weight loads, whilst the tibiofemoral joint is subject to 1-2 times body weight.
- Avoidance of provocative environments. Although difficult, avoidance of stairs, inclines etc can help when recovering from acute exacerbations.
- Physiotherapy;
- Optimise quadriceps function
- Assist with patello-femoral maltracking with taping
- Ensure hamstring and other muscle groups are supple
Operative
As in most orthopaedic conditions, surgery is usually only performed after a failure of non-operative measures. Surgery is always combined with a comprehensive physical therapy regime.
- Arthroscopy and lateral release: There is a very limited role to arthroscopy alone. If there is debris or a loose body, arthroscopy alone may be indicated. Combining a lateral release with arthroscopy has been performed, however, extensive lateral release defunctions the Vastus lateralis and can unbalance the quadriceps mechanism further.
- Tibial Tuberosity Transfer: This operation aims to unload the PFJ by lengthening the quadriceps lever arm, which reduces joint reaction force through the PFJ. This operation often reduces pain and restores extensor mechanism function. In this surgery the tibial tuberosity is moved anteriorly and medially to improve tracking and unload the PFJ. Screws are used to stabilise the fragment until bone union occurs, usually by 6 weeks post-operative. Rehabilitation usually takes 6 months to plateau.


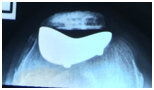
3. Isolated Patellofemoral Joint Replacement: A small number of patients are suitable for Isolated PFJ replacement. Those suitable have end stage OA, often with joint erosion, with pristine tibiofemoral articulation. The benefit of such an operation is that normal tibio-femoral kinematics are preserved, whilst the painful PFJ is rebalanced. Longer term results of this operation vary, depending upon patient selection, surgical technique and implant choice. Reflecting these complexities, the revision rate at 5 years is approximately 15% according to the AOA National Joint Replacement Registry. Other published studies report better results.

4. Total Knee Replacement (TKR): As with all end stage arthritis of the knee, TKR is a viable procedure for end stage PFJ OA. Often patients have coped with isolated PFJ pain until other elements of the knee degeneration occurs. The knee decompensates and then pain gets worse. This is a common scenario, and in the older patient is usually well managed with TKR.
